Radiofrequency and microwaves in the treatment of gynaecological pathology
Reading Time: 4 minutesAt our clinic, we are highly specialised in the diagnosis and treatment of adenomyosis.
At our department we have introduced new minimally invasive surgical methods, such as radiofrequency or microwave thermo-ablation, which is a new and revolutionary method for treating adenomyosis (you can find articles specifically dedicated to thermo-ablation in the blog).
The use of radiofrequencies and microwaves represents a new frontier in the treatment of uterine fibromatosis and is a minimally invasive procedure that allows effective treatment with minimal impact on both the clinical condition of patients and health economics.
Recent data have demonstrated the safety and efficacy of this procedure, with resolution or improvement of symptoms and significant reduction in the volume of fibroids treated. At the same time, they have demonstrated the efficacy and high tolerability of this procedure, leading to both a reduced need for re-intervention and easy post-operative management, manageable even with only the use of NSAIDs for post-operative pain. [Lee BB et al. 2016]
Uterine fibromatosis is a major problem in women's health, affecting up to 70% of Caucasian women and up to 80% of African-American women by the age of 50, and is a major indication for hysterectomy. [Day Baird D et al. 2003].
Radiofrequency treatment takes advantage of recent technological advances in instrumentation and imaging to provide a safe, effective and conservative approach to the uterus. [Lee BB et al. 2016]
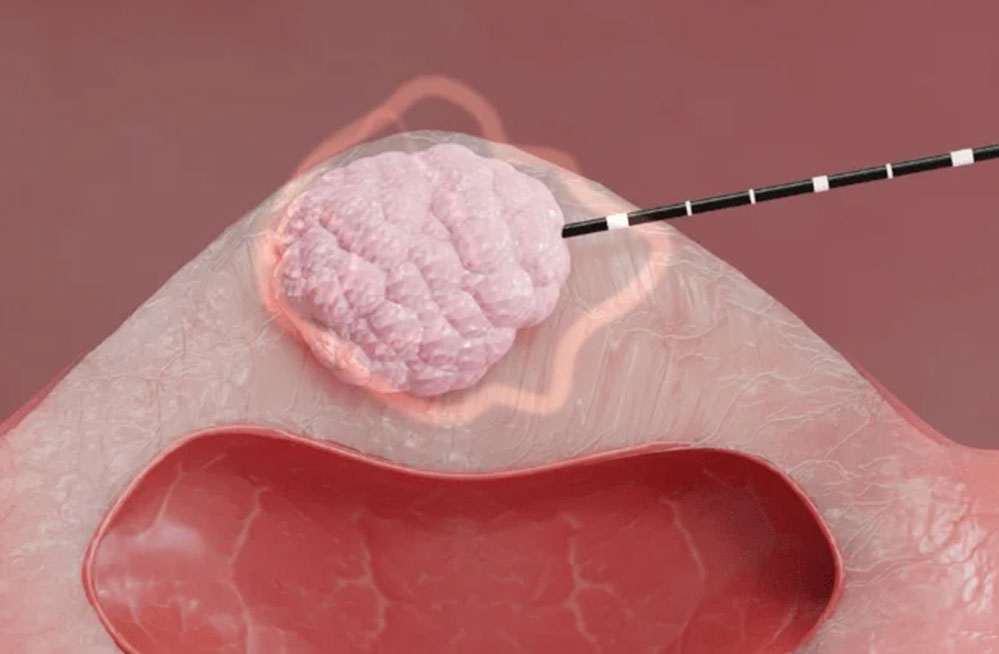
This method is based on the production of a high-frequency, low-voltage alternating current by means of an electrode that, when positioned at a target tissue, produces heat that spreads by thermal conduction, allowing its volumetric ablation by coagulative necrosis. Heat can be applied by direct thermal conduction, as in endometrial ablation by heated fluid, or by ultrasound or microwaves. [Lee BB et al.2016]
The size and shape of the ablation volume are dependent on the time taken, the maximum temperature reached and the type of electrode used. [Lee BB et al.2016]
The additional advantage of this method is that, by using frequencies typically between 450 and 500 kHz, it prevents nerve stimulation at the level of the tissue involved, which typically occurs at frequencies below 10 kHz. [Hammerich D. et al. 2006].
Microwave ablation, on the other hand, uses the creation of an electromagnetic field around an electrode that leads to an increase in local temperature and coagulative necrosis in the target tissue.
The first use of radiofrequency in the treatment of uterine fibromatosis dates back to 2002, when Lee et al. demonstrated how, in a sample of 52 patients with a total of 197 leiomyomas ranging in size from 1 to 11 cm, this method led to a reduction in fibroid volume of 36% at three months and 41% at six months after treatment, with a resolution of symptoms up to 90% one year after treatment. There were also no complications at surgery or peri-operatively. [Lee BB. et al. 2002].
During the 3-year follow-up, Lee et al. also demonstrated that 94% of the treated sample was still asymptomatic, with only one re-intervention for symptomatic fibromatosis 23 months later. [Lee BB et al. 2005]
In 2005, Lee initiated the design of a new radiofrequency ablation method, called the Acessa System, which received FDA approval for the treatment of uterine fibromatosis in 2012. [Lee BB et al. 2016]
Although evidence on the efficacy of myolysis has generally been reported using a laparoscopic approach, in 2011 Chung-Hoon Kim et al. verified the efficacy and reliability of radiofrequency myolysis using an echo-guided transvaginal approach. [Kim CH et al. 2011] In a sample of 69 women with an average age of 39.8 years with symptomatic uterine fibromatosis, data on the volumetric reduction of fibroids by ultrasound study, the degree of resolution of menorrhagia, and the overall improvement in symptoms associated with fibromatosis were analysed. All the results obtained, which confirmed a reduction in the volume of dominant myomas and an improvement in menorrhagia and associated symptoms one, three, six and twelve months after treatment, were statistically significant. [Kim CH et al. 2011].
A final very interesting fact concerns the 15 pregnancies that occurred in 13 patients with live births after radiofrequency treatment for fibroids. Of these, 14 pregnancies occurred after laparoscopic ultrasound-guided treatment, with 12 deliveries occurring at term with live, viable fetuses and 2 miscarriages in the first trimester; only one pregnancy occurred after transuterine treatment. Of these 13 total deliveries, 8 occurred by caesarean section and 5 through vaginal deliveries. [Lee B et al., 2016]
Available studies have shown low rates of complications such as intra-procedural bleeding, although the risk of adhesion formation cannot be ruled out, although it is certainly lower than the surgical approach normally used. This treatment has also shown the great advantage of not requiring general anaesthesia and requiring only one night's hospitalisation. There are to date no data in the literature on the impact of microwaves on fertility. [Ierardi et al., 2018].
In conclusion, it can be seen that the use of radiofrequency and microwave technology represents a very promising frontier in the treatment of gynaecological pathologies such as uterine fibromatosis, and more recently adenomyosis, with a good post-operative prognosis in terms of symptoms and post-operative recovery, and with significant health savings, allowing shorter operating times and a reduction in the hospitalisation of patients.
BIBLIOGRAPHY
Lee BB, Yu SP. Radiofrequency Ablation of Uterine Fibroids: a Review. Curr Obstet Gynecol Rep. 2016;5(4):318-324. doi: 10.1007/s13669-016-0183-x.
Day Baird D, Dunson DB, Hill MC, Cousins D, Schectman JM. High cumulative incidence of uterine leiomyoma in black and white women: ultrasound evidence. Am J Obstet Gynecol. 2003;188:100-107. doi: 10.1067/mob.2003.99.
Hammerich D. Tissue ablation. In: Webster JG, editor. Wiley encyclopedia of medical devices and instrumentation. New Jersey: John Wiley & Sons; 2006. pp. 362-379.
Huang K, Hong R, Luo L, Zhao H, Wang Y, Li Y, Jiang Y, Zhou H, Li F. Efficacy and safety of different thermal ablative therapies for desmoid-type fibromatosis: a systematic review and meta-analysis. Quant Imaging Med Surg. 2023 Oct 1;13(10):6683-6697. doi: 10.21037/qims-23-289.
Lee BB. Radiofrequency ablation of uterine leiomyomata: a new minimally invasive hysterectomy alternative. Obstet Gynecol. 2002;99(4s):9S.
Lee BB. Three-year follow-up post radiofrequency ablation of uterine leiomyomata. J Min Inv Gynecol. 2005;12(5s):S51. doi: 10.1016/j.jmig.2005.07.121.
Kim CH, Kim SR, Lee HA, Kim SH, Chae HD, Kang BM. Transvaginal ultrasound-guided radiofrequency myolysis for uterine myomas. Hum Reprod. 2011;26(3):5599-5563. doi: 10.1093/humrep/deq366.
Ierardi AM, Savasi V, Angileri SA, Petrillo M, Sbaraini S, Pinto A, Hanozet F, Marconi AM, Carrafiello G. Percutaneous High Frequency Microwave Ablation of Uterine Fibroids: Systematic Review. Biomed Res Int. 2018 Jan 8;2018:2360107. doi: 10.1155/2018/2360107.
Berman JM, Guido RS, Garza-Leal JG, Pemueller RR, Whaley FS, Chudnoff SG. Three-year outcome of the halt trial; a prospective analysis of radiofrequency volumetric thermal ablation of myomas. J Min Inv Gynecol. 2014;21(5):767-774. doi: 10.1016/j.jmig.2014.02.015.