Why treat uterine fibroid with thermoablation or myolysis
Reading Time: 3 minutesIntroduction
Uterine fibroids are the most common benign tumors of the female genital tract, with a prevalence of up to 70% in women of reproductive age. While many remain asymptomatic, approximately 30–40% cause clinically significant symptoms, including heavy menstrual bleeding, iron-deficiency anemia, pelvic pain, pressure-related urinary or bowel symptoms, infertility, and adverse pregnancy outcomes. Historically, hysterectomy and myomectomy were the main therapeutic approaches, but both are associated with surgical risks, longer recovery times, and partial or complete loss of reproductive potential. In recent years, minimally invasive alternatives such as thermoablation (radiofrequency, microwave, HIFU) and myolysis have gained increasing attention for their clinical efficacy and favorable safety profile.
Principles and advantages of thermoablation
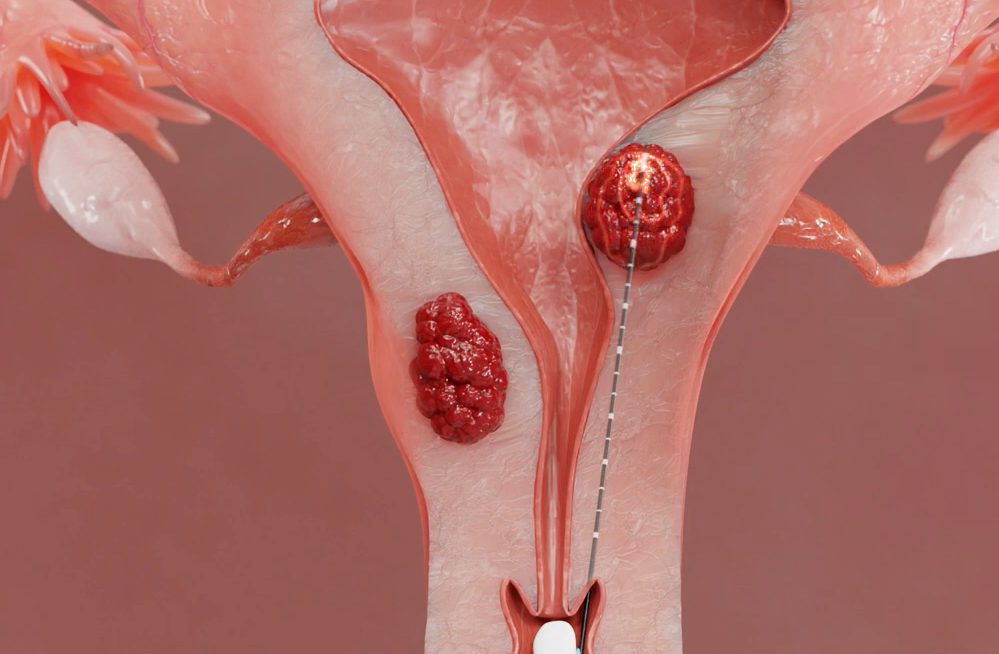
Thermoablation applies targeted thermal energy to induce coagulative necrosis of fibroid tissue, progressively leading to volume reduction. Techniques include radiofrequency, microwave energy, and high-intensity focused ultrasound. Unlike conventional surgery, thermoablation does not require large abdominal incisions and can often be performed under local anesthesia or mild sedation. Patients are usually discharged the same day and resume daily activities within a few days, offering clear advantages in terms of quality of life, reduced postoperative pain, and lower healthcare costs.
Uterine preservation and fertility outcomes
A critical advantage of thermoablation is its capacity to preserve uterine integrity, which is particularly important for women seeking future fertility. Unlike hysterectomy, which permanently eliminates reproductive potential, or myomectomy, which may weaken the myometrium and increase the risk of uterine rupture in pregnancy, thermoablation spares uterine structure. Clinical reports increasingly describe spontaneous conceptions and successful pregnancies following fibroid ablation, with reproductive outcomes comparable to surgery but achieved with less myometrial disruption.
Clinical efficacy and symptom control
Volume reduction after thermoablation is progressive, yet symptomatic improvement is often observed within weeks. Prospective studies have shown fibroid shrinkage of 50–70% at 6–12 months, alongside significant improvements in menorrhagia and anemia. Patient-reported outcomes confirm enhanced quality of life, reinforcing the effectiveness of the approach in managing both structural and symptomatic burdens.
Emerging clinical observations
Beyond gradual shrinkage, new clinical evidence suggests that fibroids may undergo an immediate reduction in size of about 10–20% directly after the procedure. Furthermore, submucosal fibroids initially classified as G2 may “migrate” toward less invasive stages (G1–G0), thereby becoming more amenable to hysteroscopic resection. This sequential strategy highlights thermoablation not only as a standalone therapy but also as a valuable adjunct in multimodal fibroid management.
Conclusions
Thermoablation and myolysis are safe and effective treatments for uterine fibroids, offering rapid recovery, reduced morbidity, preservation of uterine integrity, and potential fertility. Recent findings on immediate volume reduction and improved hysteroscopic accessibility further expand their clinical utility. Long-term prospective studies are warranted to confirm reproductive safety and refine patient selection criteria.
REFERENCES
Chen I, Berman JM, Balk EM, Saldanha IJ, Kowalczewski E, Yi J, Zanotti S, Al Hilli M, Kho KA. Radiofrequency Ablation for the Treatment of Uterine Fibroids: A Systematic Review and Meta-Analysis by the AAGL Practice Committee. J Minim Invasive Gynecol. 2025 Jan;32(1):74-91. doi: 10.1016/j.jmig.2024.09.011. Epub 2024 Sep 12. PMID: 39277104.Chen I, et al.
Jonsdottir G, Beermann M, Lanz E, Nikodell A, Cronsioe A, Hasselrot K, Kopp-Kallner H. Ultrasound guided microwave ablation treatment of uterine fibroids: Clinical response and patient acceptability. Acta Obstet Gynecol Scand. 2025 Feb;104(2):350-356. doi: 10.1111/aogs.15041. Epub 2024 Dec 19. PMID: 39697096; PMCID: PMC11782056.
Zhang Q, Liang X, Chen Z. An Updated Review of Thermal Ablation Technology for Uterine Fibroids and Adenomyosis: Focusing on Protecting Fertility. Int J Womens Health. 2024 Sep 23;16:1551-1563. doi: 10.2147/IJWH.S473005. PMID: 39346931; PMCID: PMC11430362.
Khaw SC, Anderson RA, Lui MW. Systematic review of pregnancy outcomes after fertility-preserving treatment of uterine fibroids. Reprod Biomed Online. 2020 Mar;40(3):429-444. doi: 10.1016/j.rbmo.2020.01.003. Epub 2020 Jan 9. PMID: 32081542..
Patel N, Chaudhari K, Patel D, Joshi J. High-Intensity Focused Ultrasound Ablation of Uterine Fibroids: A Review. Cureus. 2023 Sep 4;15(9):e44680. doi: 10.7759/cureus.44680. PMID: 37809132; PMCID: PMC10550780.Aviram R, et al. Advances in minimally invasive fibroid treatment: focus on ablation. J Clin Med. 2025;14(5):1621. PMID: 40228557.